Examples of Clinical Variant Interpretation with VSClinical
In this chapter, I’d like to go through a few examples for variants that have been classified with the help of VSClinical. This will give you a better understanding of how data sources are actually being represented in the software and how those are used to make decisions on applicable criteria. It goes without saying that having the relevant information embedded in a clinical workflow solution helps to streamline the clinical evaluation process by avoiding any type of paradigm or platform shifts.
Benign Frameshift Variant MSH6 p.K1358Dfs*2
Let’s begin with a simple benign variant. MSH6 c.4068_4071dupGATT (p.K1358Dfs*2) is a great example of a variant you might evaluate that turns out to be benign. At first glance, this variant is rare in the global population catalogs. However, it is seen at a frequency of 3.3% in East Asians in the gnomAD exome dataset, as well as occurring in 10 total individuals in a homozygous genotype state.
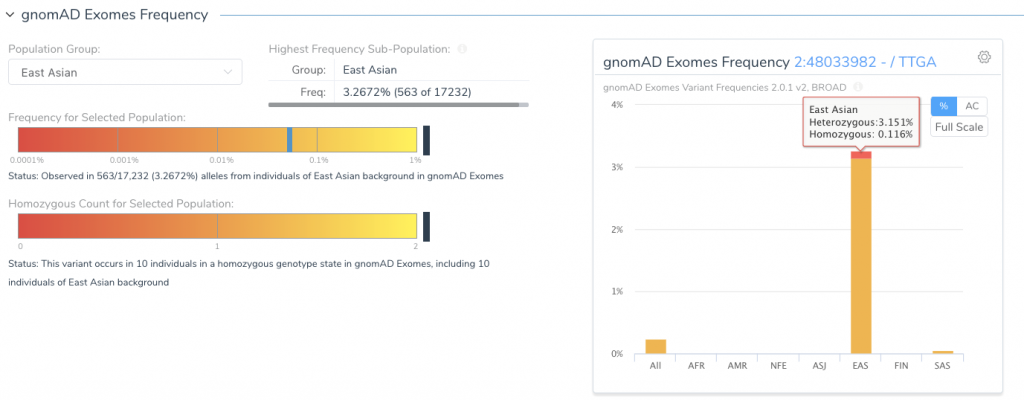
With this starting point, the variant would require significant clinical or functional evidence of being pathogenic to consider further. Although this variant is a frameshift variant that potentially truncates the gene, it does not meet the requirements for being scored as a null variant. For these reasons, the guidelines workflow recommends a benign classification for this variant.
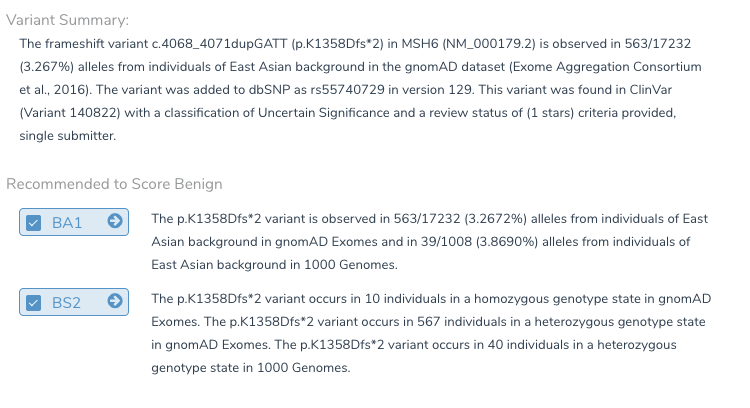
Table 2: The Super fams criteria for this benign variant.
Pathogenic Missense Variant RAF1 S257L
Now, let’s look at the other side of the spectrum. We will evaluate the c.770C>T (p.S257L) mutation in RAF1. This gene is associated with Noonan Syndrome, inherited in an autosomal dominant model and often resulting in some form of critical congenital heart disease. In comparison to the previous variant, this missense variant has many pathogenic criteria recommended. We will briefly cover each recommendation and investigate the provided evidence before choosing to accept the recommendation and score each criterion.
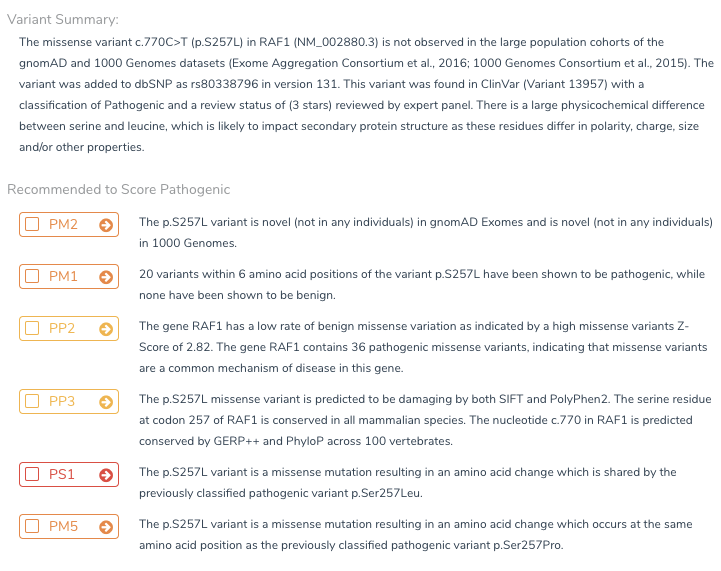
Because this variant is novel (not present in either the 1,000 genomes or gnomAD catalogs), the PM2 criteria can be objectively applied.
Moving onto the criteria related to the gene impact and function, we must evaluate whether this missense is in a mutation hotspot (PM1). In VSClincial, the PM1 scoring question is preceded by a table of previously classified variants of the same type and in the same region. The automated analysis reports that there are 18 known pathogenic neighbor variants within 6 amino acids of the variant position and no classified benign variants. This provides the confidence to answer the questions that result in PM1 being scored.
To continue reading the classification criteria of pathogenic variants, please download a complimentary copy of “Clinical Variant Analysis” by clicking on the button below.